
Is It Patch-Worthy?
The patch shortage is real. The panic is optional. I've got a tool for you.

In 1995, Elaine Benes had a crisis.
Her beloved Today Sponge (a contraceptive sponge, for the younger readers) was being pulled from the market. So Elaine did what any rational woman would do. She scoured every pharmacy in a 25-block radius, bought a lifetime supply, and then developed a rigorous screening process to determine which of her dates were “sponge-worthy.” It remains one of the greatest Seinfeld episodes of all time. It’s also, suddenly, very relatable.

If you’re a woman on an estradiol patch in 2026, you know the drill. You go to the pharmacy. They tell you it’s on backorder. You try CVS. Walgreens. The sketchy independent pharmacy across town with the flickering fluorescent light. You call your doctor’s office in a mild panic. You ask your friends if they have an extra. You consider cutting your patch in half (that will work, but now you’ve got half the dose). You are Elaine Benes, minus the sponge, plus a hot flash.
The estradiol patch shortage is real, and it’s everywhere. Climara, Vivelle-Dot, Dotti, generics from Teva and Mylan. All in short supply, some on indefinite backorder. PBS NewsHour, CNN, NPR, and NBC have all run stories. Your group chat has probably discussed it more than once.
First, we’ll discuss “the why” and then we’ll get to “what the heck do I do about it?”
Note: At the end of this article, I’m sharing the link to an Estradiol Swap Tool, a free digital tool I built to help you find the best alternative to your current patch dose and the lowest cash price. I really outdid myself this time! :)
Why Is This Happening?
Three things collided at once. And at least one of them traces back directly to the man currently occupying the Oval Office.
First, demand. This is the good-news part. Prescriptions for estrogen have risen roughly 86% over the past five years, and about half are for patches. The biggest acceleration happened after the FDA removed the black box warning from menopausal hormone therapy products. That warning, slapped on estrogen after the Women’s Health Initiative results in 2002, overstated the risks and scared an entire generation of women (and their doctors) away from hormones. When it came off, women flooded their doctors’ offices asking for the patches they’d been told for twenty years would kill them. This is genuinely wonderful. More women getting hormones is exactly what I’ve been fighting for.
Second, a manufacturing bottleneck. The estradiol molecule is widely available. It’s the same 17-beta estradiol whether it’s in a patch, a gel, a cream, a ring, or a pill. The shortage is not really an estradiol shortage. It’s a patch shortage. And that distinction matters.
A transdermal patch is a multi-layer engineered device. It requires specialized pressure-sensitive adhesives (acrylic, silicone, or polyisobutylene-based), polymer backing films (PET, polyethylene, EVA), rate-controlling membranes, and release liners. You can’t just pour estradiol into a Band-Aid. These are engineered drug delivery systems with specific absorption rates, adhesion properties, and stability requirements. There are only a handful of facilities worldwide that produce this technology, and scaling up production takes years. Sandoz has specifically reported adhesive problems with its patches as a contributor to shortages.
Third, tariffs. About 80% of the active pharmaceutical ingredients used in generic drugs in the United States are manufactured overseas, primarily in China and India. Even though estradiol patches are classified as generics and are currently exempt from pharma-specific tariffs, the industrial materials used to build the patch delivery system are not. Tariffs on specialized polymers used in adhesive backings, aluminum foils, and release liners are elevating input costs for domestic patch manufacturers. When you’re already operating on razor-thin generic margins and your raw material costs go up, you don’t invest in new production lines. You make less. Or you stop.
In 2025, the Trump administration rolled out sweeping “reciprocal” tariffs and Section 232 tariffs on pharmaceutical ingredients, finished medications, and the raw materials used to make them. Last week, Trump and his band of dysfunctional sycophants imposed a 100% tariff on patented pharmaceutical imports from companies that haven’t signed “reshoring” deals with the Commerce Department. Generic drugs were technically spared (for now), but the executive order states the Commerce Department will “re-evaluate generics tariffs” within a year. That goal of bringing drug manufacturing back to the U.S. is a fantasy on this timeline. You cannot rebuild domestic manufacturing capacity in months. Industry experts say it would take 2 to 3 years, or longer, for complex formulations like transdermal delivery systems. In the meantime, tariffs raise input costs for manufacturers who were already barely incentivized to make these products. When it becomes unprofitable to make a product, manufacturers stop making it. Or they make less. Or they raise prices. All three are happening right now with estradiol patches
Should You Freak Out?
No.
You found the thing that works. You fought for it. You felt like yourself again for the first time in years. And now the pharmacy is telling you they can’t fill it. That’s maddening. But it’s not a crisis. It’s an inconvenience, and there are excellent alternatives.
Things to think about…
Size matters
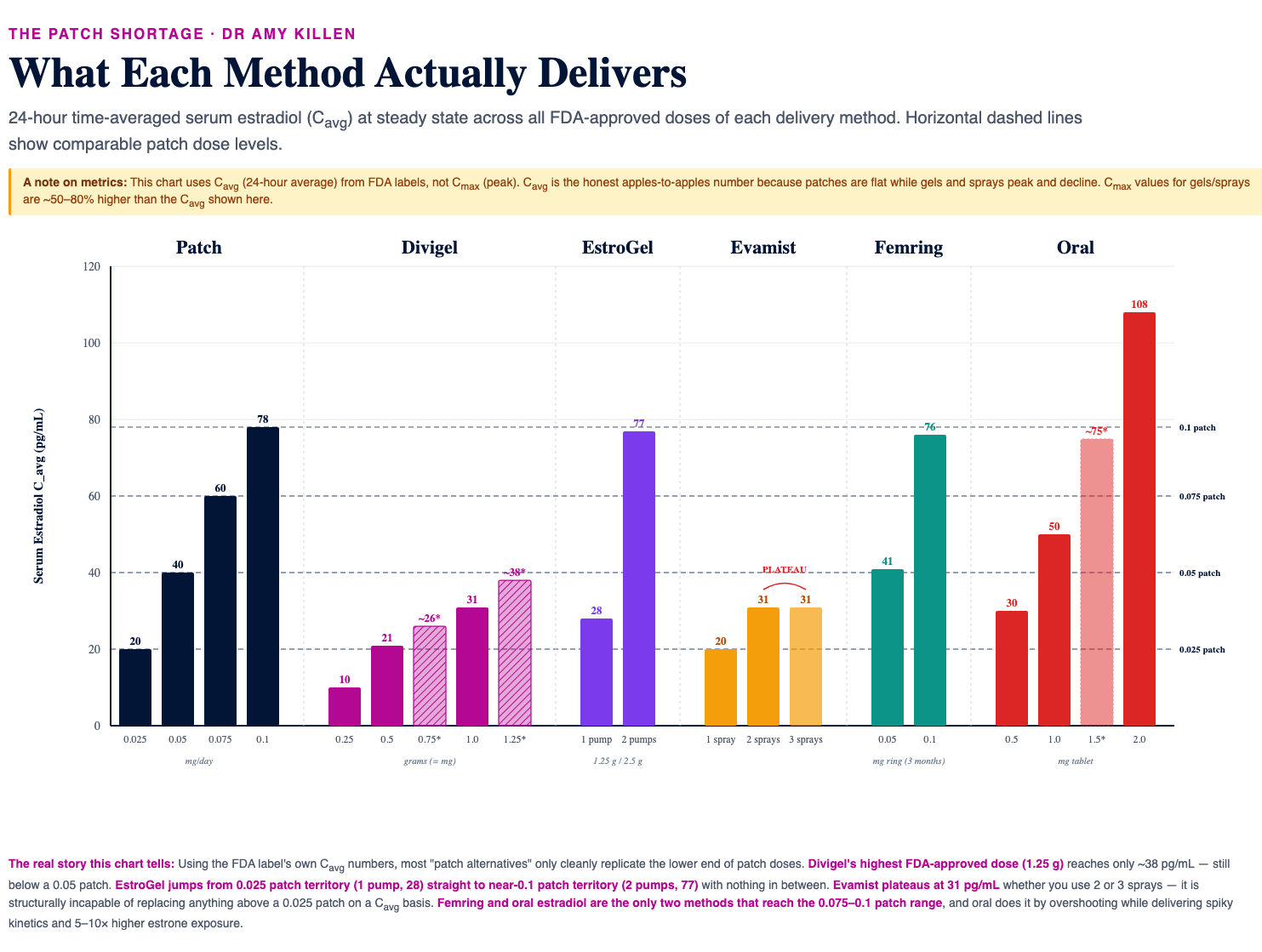
Not all estradiol formulations are created equal, but several produce blood levels and stability comparable to the patch. I’ve made some graphics comparing median serum estradiol levels across formulations, which you’ll find below. Find your patch dose (black bars) and compare it with other products.
As you’ll see, if you’re on a higher-dose estradiol patch (think: 0.75 - 0.1 mg/day), estradiol sprays (like Evamist) are not going to get you where you need to be. The peak serum estradiol levels after 2-3 sprays of Evamist only hit 55 pg/mL, and the average serum estradiol levels are a paltry 30 pg/mL, which is basically a midlife man’s serum estradiol level.
It’s not (just) the size of the boat, it’s the motion of the ocean
Median estradiol level is only half the story. The other half is stability. How smooth is the ride? One of the big benefits of patches is that serum estradiol levels stay remarkably consistent over time. You don’t get the big highs and lows you might get from other forms. That consistency isn’t necessary for good results, but women who are very sensitive to fluctuations (think: histamine intolerance, migraines, significant drug sensitivities) may notice.
Think about this like the ocean.
Estradiol patches are flat water. We’re talking glassy, not-a-ripple, attempting-yoga-balance-poses-on-a-stand-up-paddleboard kind of flat. You slap a patch on, and your estradiol level stays remarkably consistent until you change it. Femring is the same story. You insert it and forget about it for three months. Three months of glass. No weekly patch changes, no adhesive rashes, no peeling edges during your workout. The fact that more women don’t know about Femring as a systemic estrogen option is a failure of medical education, in my opinion. (The downside is cost. Around $900 to $1,100 per ring without insurance, and there’s no generic. But if your insurance covers it, Femring is arguably the most elegant alternative to the patch.)
Gels (EstroGel, Divigel, Elestrin), sprays, injections, and oral estradiol are going to give you some waves (or, in the case of injections, a peak and slow, steady decline). You’ll see a rise after each dose and a dip before the next one. But once you reach steady state (usually within a couple of weeks of consistent dosing), most women don’t notice the chop. The skin acts as a reservoir with gels, smoothing things out. Oral estradiol taken daily at the same time produces a predictable rhythm. Think mild ocean, maybe a foot or two. For the vast majority of women, the clinical experience with gels or oral is indistinguishable from the patch.
The Bottom Line
If you’re on a patch and can’t fill it, don’t sit at home rationing your last patch like Elaine with her sponges. Call your prescriber. Ask about Femring, gels, injections or (if you’re otherwise healthy) oral estradiol.
The patch shortage is real, and it’s not going away anytime soon. But, you’ve got choices and work-arounds (which is more than I can say for the gas shortage that our fine president is getting us into as we speak… 🙁)
Speaking of which (patches, not gas), I’ve got something very cool to share with you. I’ve created (with my very own hands!) a free digital tool called the “Estradiol Swap Tool” where you can search for the best alternatives for you based on your current patch dose and your budget. It’s totally free - you just need to venture over yonder to my website and put in your email.
Comments? Concerns? I’m happy to hear what you have to say - about the patch shortage, the gas shortage and anything else this article might have covered. And, while I respect your right to a different opinion than me, I will not tolerate rude or abusive remarks. I feel like that should go without saying, right?
Sources:
FDA Femring Prescribing Information (estradiol acetate vaginal ring)
FDA Evamist Prescribing Information (estradiol transdermal spray)
Brennan JJ et al. Serum concentrations of 17beta-estradiol and estrone after multiple-dose administration of percutaneous estradiol gel. Ther Drug Monit. 2001;23:134-8.
Järvinen A et al. Comparative absorption and variability in absorption of estradiol from a transdermal gel and a novel matrix-type transdermal patch. Maturitas. 2001;38:189-196.
Morton TL et al. Steady-state pharmacokinetics following application of a novel transdermal estradiol spray in healthy postmenopausal women. J Clin Pharmacol. 2009;49:1037-1046.
Newson Health clinic cross-sectional study, PMC (2023 data, published 2025)
AJMC, “How Trump’s Trade Policy Could Raise Costs, Deepen Drug Shortages,” March 2026
Paloma Health, “How Drug Tariffs Could Drive Up the Cost of Thyroid, HRT, and GLP-1 Medications,” 2025
White House Fact Sheet, “Adjusting Imports of Pharmaceuticals,” April 2, 2026
White House Presidential Action, “Adjusting Imports of Pharmaceuticals and Pharmaceutical Ingredients into the United States,” April 2, 2026
NPR, “Menopause hormone therapy is in short supply at some pharmacies,” March 10, 2026
NPR, “What’s ahead for the weight-loss drugs known as GLP-1s in 2026,” January 1, 2026
19th News, “Impacted by the estrogen patch shortage?” February 27, 2026
NBC News, “Estrogen patch shortages are getting worse,” April 10, 2026
PBS NewsHour, “Estrogen patches face shortage,” April 7, 2026
CNN, “Estrogen patch shortage as demand for menopause hormone therapy grows,” February 23, 2026
CNBC, “Trump administration sets up to 100% tariffs on some imported drugs,” April 2, 2026
Tax Foundation, “Trump Pharma Tariffs Would Raise Drug Prices for Americans,” August 2025
U.S. Energy Information Administration, Short-Term Energy Outlook, April 2026
IEA Oil Market Report, March 2026
ASHP Drug Shortage Database (progesterone, testosterone cypionate, estradiol patches), accessed April 2026
Medfinder, “Progesterone shortage: What providers and prescribers need to know in 2026,” February 2026
Medfinder, “Testosterone Shortage Update,” February 2026
Contrary Research, “How GLP-1s Broke Healthcare Distribution,” January 2026
As someone who exists in a hot tub daily, I’ve traded in my patch for gel. 2 pumps. One earlier in the day. And one later. I don’t think I absorb it as well as I did the patch. But it’s good enough for me.
Long live estrogen.
They will pry my oral estradiol from my cold 🥶 ☠️ 🙌 haha. Great article!