

Last week, researchers at Penn dropped a number worth your attention. In a study of more than 110,000 women, the ones taking a GLP-1 drug were diagnosed with breast cancer about 30% less often than the ones who weren’t. Thirty percent. For the most common cancer in women.
That’s the kind of number that launches a thousand group chats. It’s also a number worth understanding properly, because the headline version (”Ozempic prevents breast cancer!”) isn’t quite what the study says, and the real story is more useful anyway

So let’s get into the two questions women keep asking me, in the comments and the DMs and after every talk. First: “If I’m on a GLP-1, am I less likely to get cancer?” And second, usually from women with a family history that scares them: “If I do get cancer, will being on one slow it down?”
A while back, in 10 Things You Didn’t Know About GLP-1s, I covered the safety version of this question: do these drugs cause cancer? Short answer, the one that matters: no meaningful human signal, the thyroid black box is a rodent-dose precaution (the same way the old estrogen black box was more politics than data), and we actually see lower rates of some cancers in people taking them. That question is mostly settled and mostly reassuring.
This is the next question. Not “do they cause cancer,” but “might they prevent it.” And the real answer is: it depends. It depends on which woman is asking. So find yourself below.
First, the real question
When women ask whether GLP-1s protect against cancer, they’re usually asking one of two things without realizing it. Either these drugs have a direct cancer-fighting effect, or the benefit is just a downstream effect of weight loss. That difference is everything, because it decides whether the protection applies to you. If it’s purely weight loss, a woman who doesn’t need to lose weight gets nothing. If the drug does something more, on inflammation and the immune system, then even lean women might benefit.
I made the full case both ways in The People v. Microdosing GLP-1s (written as a courtroom trial, because the question really is that contested). Cancer is where it stops being a fun thought experiment. So let’s sort you into your group, then come back to it.
Group One: You’re carrying extra weight (and this is your moment)
If you’re overweight or obese, the 2026 data is genuinely exciting, and it’s mostly about you. This is the best-studied group, and the studies keep landing.
Start with that breast cancer headline I opened with. Look at who was actually in the study: women with a BMI of 25 or higher. In other words, this group. That 30% is your number, not a general one. (It held up in both Black and White women, too.)
Now “30% less” sounds dramatic, but the absolute number is calmer: about seven fewer breast cancers per thousand women. Real, worth knowing. Not a force field.
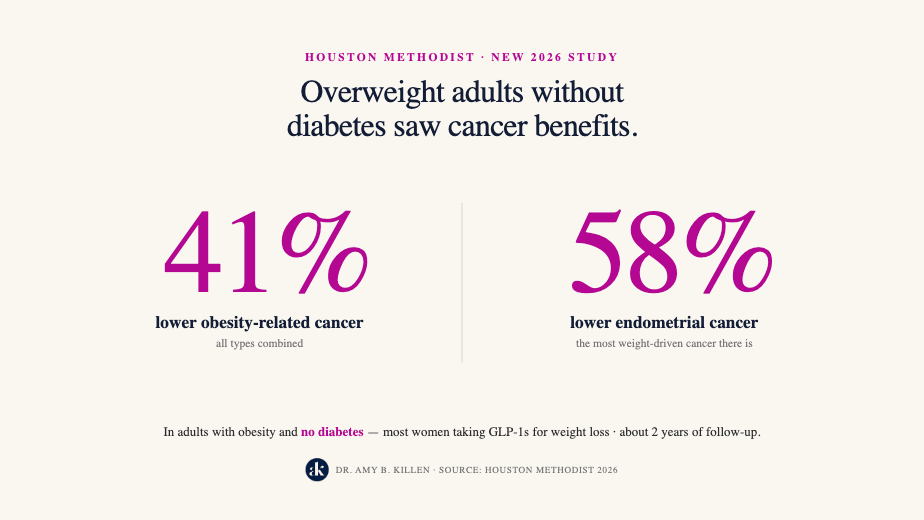
It’s not just breast cancer, either. A brand-new study out of Houston Methodist was the first to look specifically at people who are obese but not diabetic, which describes most women taking these drugs for weight loss. Over about two years, GLP-1 use was tied to a 41% lower rate of obesity-related cancers overall, and endometrial cancer, one of the most weight-driven cancers there is, dropped by 58%.
And for your group, a lot of this protection is the weight loss itself, doing exactly what we’d hope. Fat tissue isn’t inert. It behaves like a little hormone factory, churning out its own inflammatory estrogen (estrone) and driving up insulin, both of which feed cancers like breast and endometrial. Lose the excess fat, and you turn that factory down. (This, by the way, is a completely different thing from the body-identical estradiol we use in menopause care. Adipose estrogen made in inflamed belly fat is not the same as hormone optimization therapy. Don’t let anyone conflate the two.)
So your answer is the cleanest “probably yes” in this whole article, and the reason is encouraging rather than mystical: the drug is helping you shed the exact tissue that was raising your risk in the first place.
Group Two: You have diabetes (but the fine print matters)
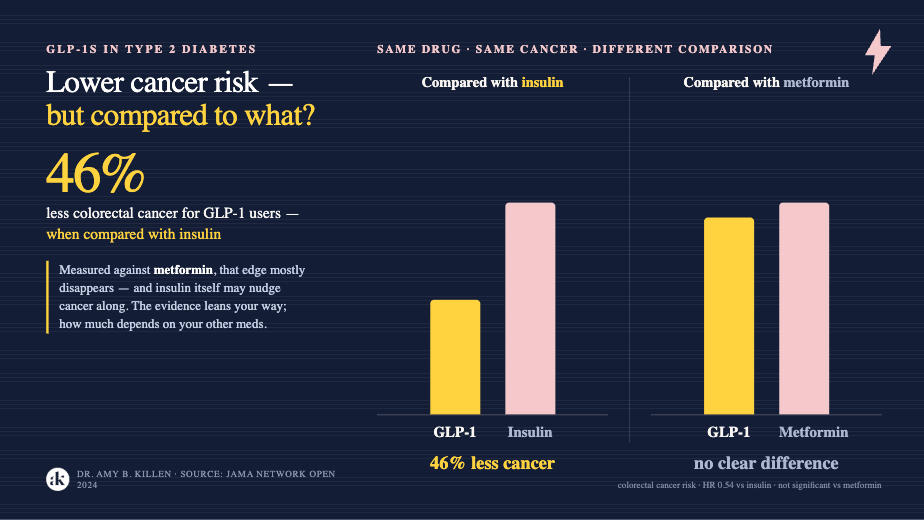
If you’re diabetic, you’ve actually been studied the longest. Big database studies show GLP-1 users develop several cancers less often, including a striking drop in colorectal cancer.
There’s a catch worth knowing. A lot of those dramatic numbers come from comparing GLP-1s to insulin, and insulin itself may nudge some cancers along. Compare GLP-1s to metformin instead, and the advantage mostly shrinks. So your takeaway is “the evidence leans in your favor, but how much depends on what you’d otherwise be taking.” Worth a real conversation with whoever manages your diabetes, not a reason to panic or to celebrate.
Group Three: You’re at a healthy weight
If you’re lean, metabolically healthy, and not diabetic, the answer is simpler and less satisfying: we have essentially no cancer data on you.
Every major study, the breast one, the Houston one, all of them, was done in people who were overweight, obese, or diabetic. Nobody has studied normal-weight women on these drugs and tracked their cancer outcomes. So when a clinic implies a slim woman should take a GLP-1 to prevent cancer, they are well out ahead of the evidence.
Could there be a benefit anyway? Maybe. As I argued in the microdosing piece, GLP-1 receptors are on immune cells and blood vessel linings, not just fat, and some of the protection in obese people seems to begin before weight loss and persist beyond it (more on that in a second). And some “normal weight” women are actually carrying inflammatory visceral fat the scale never shows. But “it might work through mechanisms we can describe” is not “it prevents cancer in lean women.”
And the math is genuinely different for you. The biggest chunk of the observed cancer benefit comes from losing excess fat you don’t have to lose. So you’d be taking on the cost, the GI side effects, the muscle and bone considerations I’m always nagging about, in exchange for a cancer benefit that is, for your body, entirely theoretical. Cancer prevention is not a reason for a healthy-weight woman to start a GLP-1. If you’re on one for another reason, fine, but don’t let anyone sell you the cancer angle. There’s nothing there yet.
So, weight loss or something more?
Both. And which one matters most depends on the cancer.
For breast and endometrial cancer, it’s mostly the weight loss. These are heavily driven by the estrogen and insulin produced by excess fat, so when the fat comes off, the risk follows it down. Nothing mysterious required.
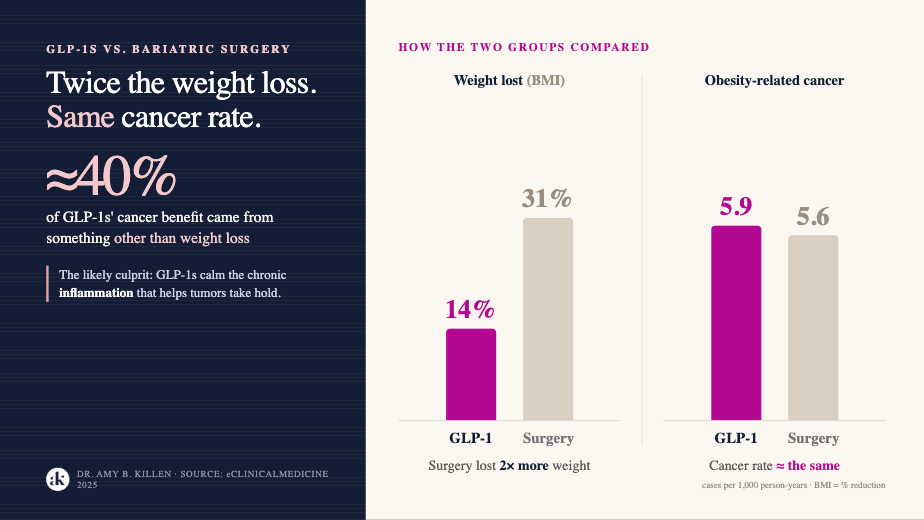
For colorectal cancer, there’s a real sign of something beyond weight loss, and the study that shows it is clever. Researchers compared people on GLP-1s to people who’d had bariatric surgery. The surgery group lost more than twice as much weight. If weight loss were the whole story, they should have ended up with far less cancer. Instead, the two groups landed in about the same place, and when the numbers were crunched, roughly 40% of the GLP-1 group’s protection came from something other than the pounds.
Think of it like two students studying for the same exam. One studies twice as long as the other, and they walk out with the same grade. The extra study time clearly isn’t the only thing driving that score. Something else is going on with the second student. With GLP-1s, that “something else” is probably the drug quieting the chronic inflammation that helps tumors take hold.
Same drug, different engine depending on the cancer. For some, it’s the weight loss. For others, it’s more than that.
“Will it slow my cancer down if I already have it?”
This is the second question women ask me, and the evidence here is much younger and much thinner, so hold it loosely.
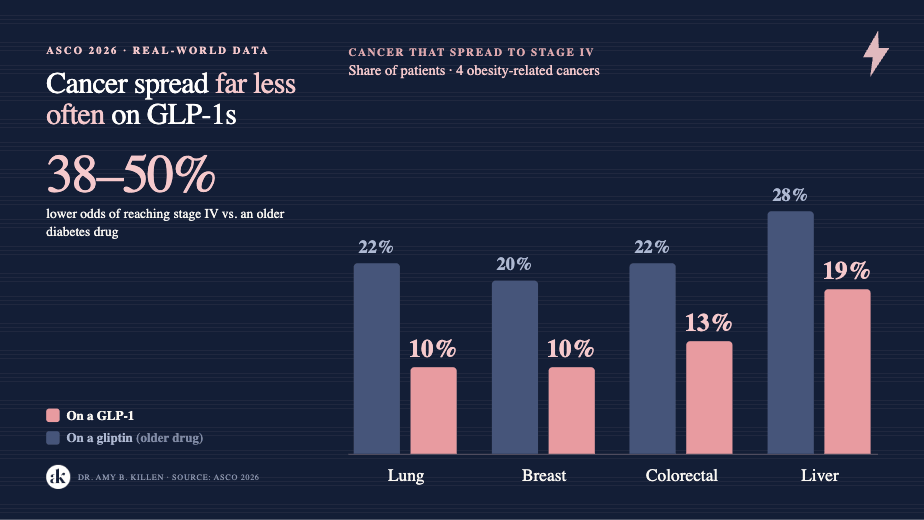
There are early signals that GLP-1s might slow how fast certain cancers spread. In one 2026 analysis, women with earlier-stage breast cancer who were on a GLP-1 were less likely to progress to advanced disease than women on a different drug. Broader real-world data hints at a slower spread in breast, colorectal, lung, and liver cancers. Interesting. Mechanistically plausible. Nowhere near settled, and absolutely not a reason to swap any part of actual cancer treatment. If you have cancer, your oncologist runs the show. Full stop.
What we still don’t know
Two caveats worth keeping in view.
First, almost all of this is observational. It shows that GLP-1 users tend to get less cancer, not that the drug caused it. When researchers pool the gold-standard randomized trials, they mostly find little or no effect on overall cancer risk. That gap, between the strong real-world signal and the quieter trial data, is where the science sits right now. It isn’t resolved.
Second, one cancer keeps showing a small uptick across studies rather than a drop: kidney cancer. Probably minor. Still being watched.
The bottom line
If you’re carrying extra weight, the cancer news is good and it’s getting better, and the beautiful part is that the protection is mostly your own body getting healthier, not a drug doing something you can’t see. If you’re diabetic, the evidence leans your way with an asterisk. If you’re lean, the answer is “we don’t know.”
But here’s the line I’ll keep repeating until I’m hoarse: the drug creates the opportunity. What you build on it is still up to you. Some of the cancer benefit is the weight itself coming off, which pulls down the estrogen and insulin that feed these tumors. And some of it looks like the drug working directly, cooling the chronic inflammation that lets cancer get a foothold, a piece that may not care what you weigh at all. That second part is why I won’t call this “just weight loss,” and why even a lean woman might turn out to benefit in ways we’re still learning to measure. The GLP-1 is a multiplier, not a magic wand.
Get your breast screening (and colonoscopies!). Lift the weights. Eat the rainbow. Take your hormones. And if a GLP-1 fits your picture, let it amplify the foundation, not substitute for it.
What group did you land in, and did anything here surprise you? Tell me in the comments. I read every one.
Standard disclaimer: I’m a physician, but I’m not your physician. This is education, not a prescription. Work with someone who knows your full picture.

References
McDonald ES, Gillis LB, Gabriel P, et al. “GLP-1 Agonists Are Associated With a Significant Reduction in Breast Cancer Incidence in Women.” JCO Oncology Practice. Published online June 2, 2026. doi:10.1200/OP-26-00485. Presented at the 2026 ASCO Annual Meeting (Abstract 10506).
Hsu AH-C, et al. (Kamat AA, senior author). “GLP-1 receptor agonist use and cancer risk in obese nondiabetic adults.” Annals of Oncology. 2026. doi:10.1016/j.annonc.2026.04.013. (TriNetX target trial emulation; 41% lower obesity-related cancer incidence over ~2 years; 58% reduction in endometrial cancer.)
Dai H, Li Y, Lee YA, et al. “GLP-1 Receptor Agonists and Cancer Risk in Adults With Obesity.” JAMA Oncology. 2025;11(10):1186-1193. doi:10.1001/jamaoncol.2025.2681. (OneFlorida+ cohort; overall cancer HR 0.83.)
Wolff Sagy Y, Ramot N, Battat E, et al. “Glucagon-like peptide-1 receptor agonists compared with bariatric metabolic surgery and the risk of obesity-related cancer: an observational, retrospective cohort study.” eClinicalMedicine. 2025;83:103213. doi:10.1016/j.eclinm.2025.103213. (Clalit; estimated ~41% direct, weight-loss-independent effect.)
Wang L, Xu R, Kaelber DC, Berger NA. “Glucagon-like peptide 1 receptor agonists and 13 obesity-associated cancers in patients with type 2 diabetes.” JAMA Network Open. 2024;7(7):e2421305. doi:10.1001/jamanetworkopen.2024.21305.
Wang L, Wang W, Kaelber DC, Xu R, Berger NA. “GLP-1 Receptor Agonists and Colorectal Cancer Risk in Drug-Naive Patients With Type 2 Diabetes, With and Without Overweight/Obesity.” JAMA Oncology. 2024;10(2):256-258. doi:10.1001/jamaoncol.2023.5573. (Online December 7, 2023; lower colorectal cancer risk vs insulin, observed with and without obesity.)
Mandala A, Unlu S, de Almeida Sartori F, et al. “Can GLP-1 receptor agonists mitigate cancer progression? A propensity-matched analysis across seven solid tumors.” Journal of Clinical Oncology. 2026;44(16_suppl):3143. Presented at the 2026 ASCO Annual Meeting (Abstract 3143; Mark D. Orland named lead/presenting author in ASCO materials). (Breast progression to stage IV 10% vs 20% versus DPP-4 inhibitor.)
American Society of Clinical Oncology. “GLP-1s May Reduce Metastatic Progression of Certain Obesity-Related Cancers.” ASCO press release, 2026 Annual Meeting. (Press summary of Abstract 3143 above.)
Silverii GA, Marinelli C, Bettarini C, Del Vescovo GG, Monami M, Mannucci E. “GLP-1 receptor agonists and the risk for cancer: a meta-analysis of randomized controlled trials.” Diabetes, Obesity & Metabolism. 2025;27(8):4454-4468. doi:10.1111/dom.16489. (50 RCTs; no significant difference in overall cancer risk, MH-OR 1.05.)
Ko A, Chang YC, Bahar F, et al. (Chiang CH, senior author). “Risk for Cancer With Glucagon-Like Peptide-1 Receptor Agonists and Dual Agonists: A Systematic Review and Meta-analysis.” Annals of Internal Medicine. 2026;179(2):216-229. Epub December 9, 2025. doi:10.7326/ANNALS-25-02237. (48 placebo-controlled RCTs, 94,245 participants; little or no effect on obesity-related cancer risk.)
Thank you for cleaning up that headline. My weight has always been healthy so no need for me to take a GLP, but I am intrigued by its anti inflammatory properties. I’m always interested in that component for taking a GLp for someone that’s generally healthy.
I definitely had insulin resistance since my 1989 pregnancy, but nobody but me ever diagnosed it.
These meds have taken care of it. Nearly 90 pounds gone. Also gone: all kinds of things that I had attributed to aging.
I will add: I did not change my diet at all. My diet of mostly home-cooked food was never the problem.