

I get some version of this question almost every week. A woman in her late sixties whose doctor just retired. A 74-year-old whose best friend won’t stop talking about how hormones gave her life back. An 80-year-old who is simply done getting a bladder infection every other month. They all ask the same thing, usually in a slightly embarrassed whisper, like they’re asking whether they can still get into a club that closed years ago. “Is it too late for me?”
No. It is not too late. (I’ll keep saying it until it sticks.)
But here’s the part nobody bothers to explain, and it’s the whole ballgame. Starting hormones at 70 is not the same conversation as starting them at 50. The type of hormone matters more, and what you can reasonably expect from it depends entirely on what you’re chasing. So let’s actually walk through it, because you deserve better than “you’re too old now,” which is both lazy and wrong.

What are the common side effects?
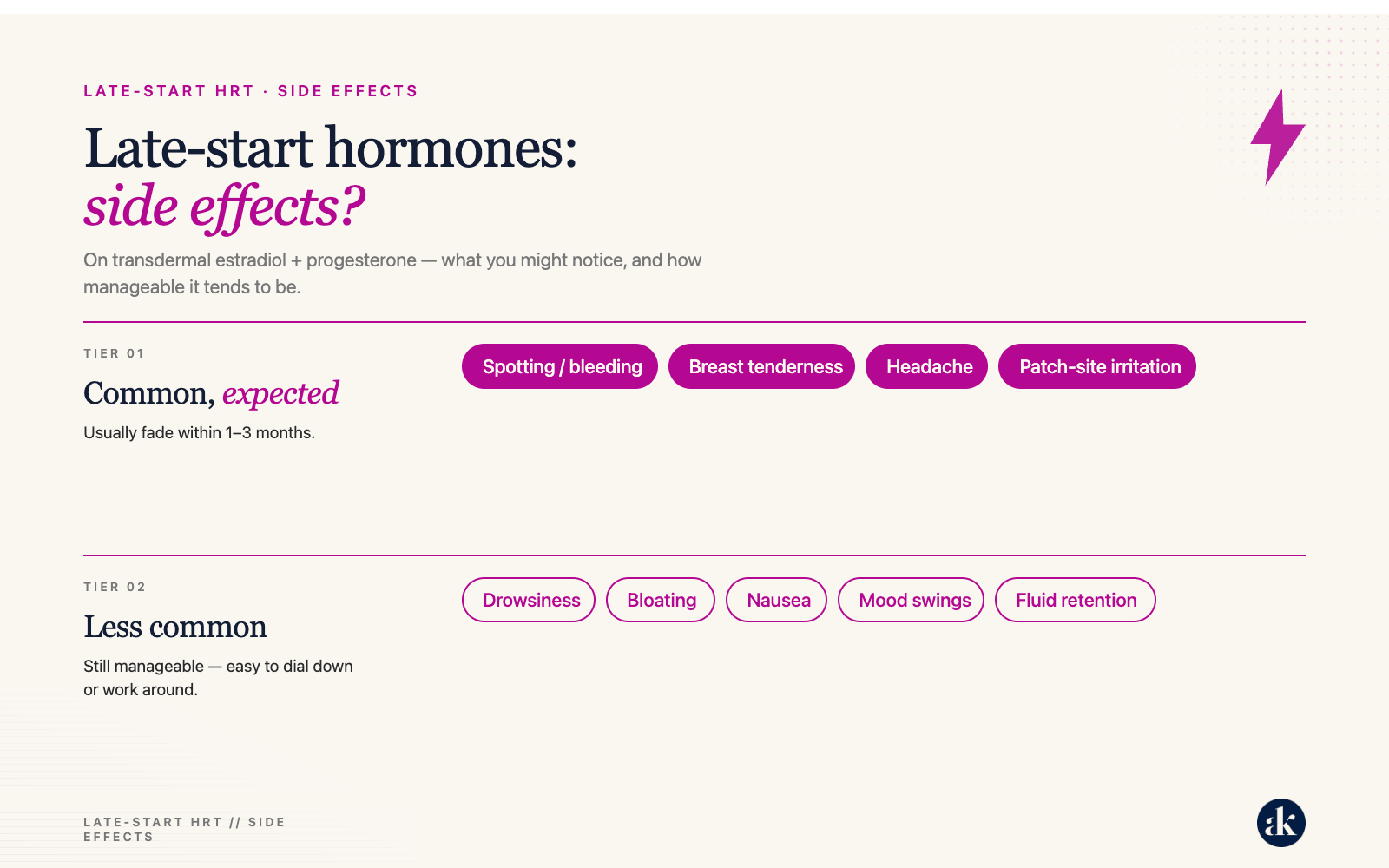
First, a reframe that makes everything else click. When women hear “hormones,” they hear “risk.” Heart attack, stroke, clot, the whole terrifying menu we were handed in 2002 when one study scared an entire generation of doctors into yanking their patients off estrogen overnight. But with the right hormones, those scary risks mostly aren’t even on the table. What’s left are side effects, and side effects are a completely different animal. A risk is the thing that lands you in the ER. A side effect is sore breasts or vaginal spotting, which we fix by nudging your dose. One is a house fire. The other is a smoke detector chirping for a fresh battery. So stop weighing risks against benefits. Start weighing side effects against benefits. That’s the real math, and it’s a far less scary one.
For the most common side effects with hormones at any age, see the chart below. Most side effects improve within 3 months and are managed by adjusting hormone doses and making lifestyle changes. The most annoying/alarming side effect is vaginal bleeding. Although it’s completely normal when starting estrogen (your uterus is getting a wake-up call after slumbering for many years), it’s also the one that gets physicians a bit concerned in older women if it doesn’t resolve on its own. That may mean needing testing, like a pelvic ultrasound. So, although most of the side effects below are mild and self-limiting, starting hormones may require closer monitoring (more doctor’s visits) and potentially additional testing.
What are the safest options?
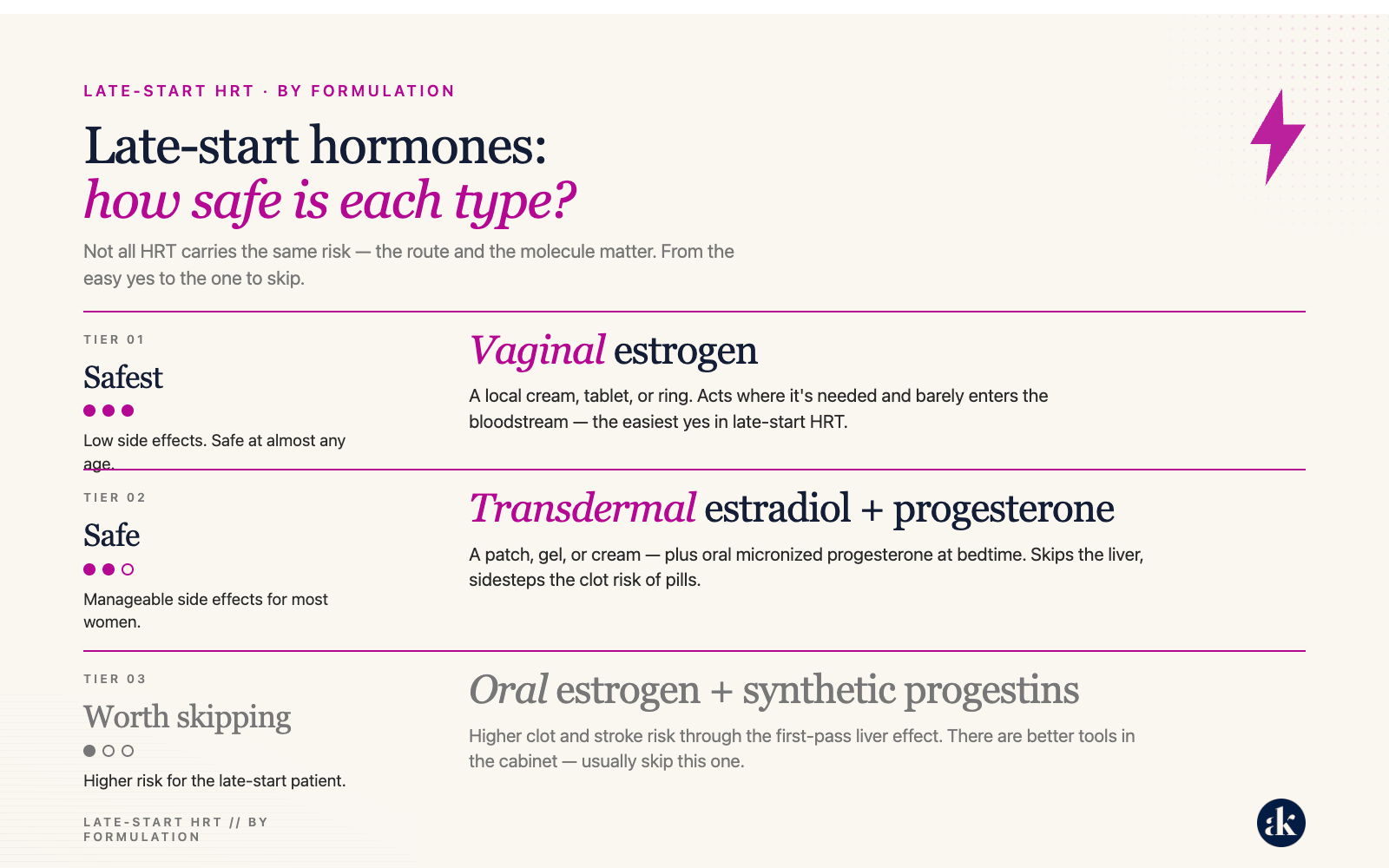
Now the hormones themselves, ranked from “yes, absolutely” down to “let’s not.”
Safest: At the very top sits the easiest yes in all of medicine: vaginal estrogen. This is a tiny dose of estradiol you put right where it’s needed, as a cream, a tablet, or a ring. It barely gets into your bloodstream, which means it skips essentially all the drama people pin on hormones. There is no age cutoff. None. I will start an 85-year-old on it this afternoon and sleep just fine tonight. It rebuilds vaginal tissue, ends the dryness and the sandpaper sex, settles a cranky bladder, and slashes those relentless UTIs. Your vagina and bladder do not care that you waited twenty years. They are simply thrilled you finally remembered they exist. If you take nothing else from this whole article, take this one thing: if you’re over 60, you are almost certainly a candidate, and almost nobody will offer it to you. So ask.
Safe: In the middle is the workhorse: transdermal estradiol paired with progesterone. “Transdermal” just means it goes through your skin, as a patch, a gel, or a cream, instead of being swallowed. That route matters more than it sounds, because swallowed estrogen takes a detour straight through your liver first, and the liver is where a good chunk of the clot risk gets cooked up. Going through the skin sidesteps the whole kitchen. You pair it with oral micronized progesterone (the real, body-identical kind, taken at bedtime) if you still have your uterus. This is safe for the vast majority of late starters. The catch, and it’s a small one, is the side effects: some breast tenderness, a little bloating, maybe spotting or a few moody days in the first few weeks. We always check out spotting just to be safe, but most of this settles on its own or vanishes the moment we tweak your dose. Annoying, sure. Dangerous, no.
Worth Skipping: At the bottom is the tier I’ll steer you away from: oral (swallowed) estrogen and the old synthetic progestins, the medroxyprogesterone “Provera” types. Swallowed estrogen takes that liver detour we just talked about, which nudges up clot and stroke risk. In a 50-year-old that risk is microscopic. In a 70-year-old starting fresh, it’s worth dodging when a patch does the same job more gracefully. And synthetic progestins are the inflammatory cousins of real progesterone, the ones tangled up in all those frightening old headlines. We have better tools now. This isn’t “never.” It’s “why on earth would we, when the nicer version is sitting right there.”
What are the potential benefits in late-starters?
So that’s safety sorted. Now the question everyone actually wants answered: will it even work?
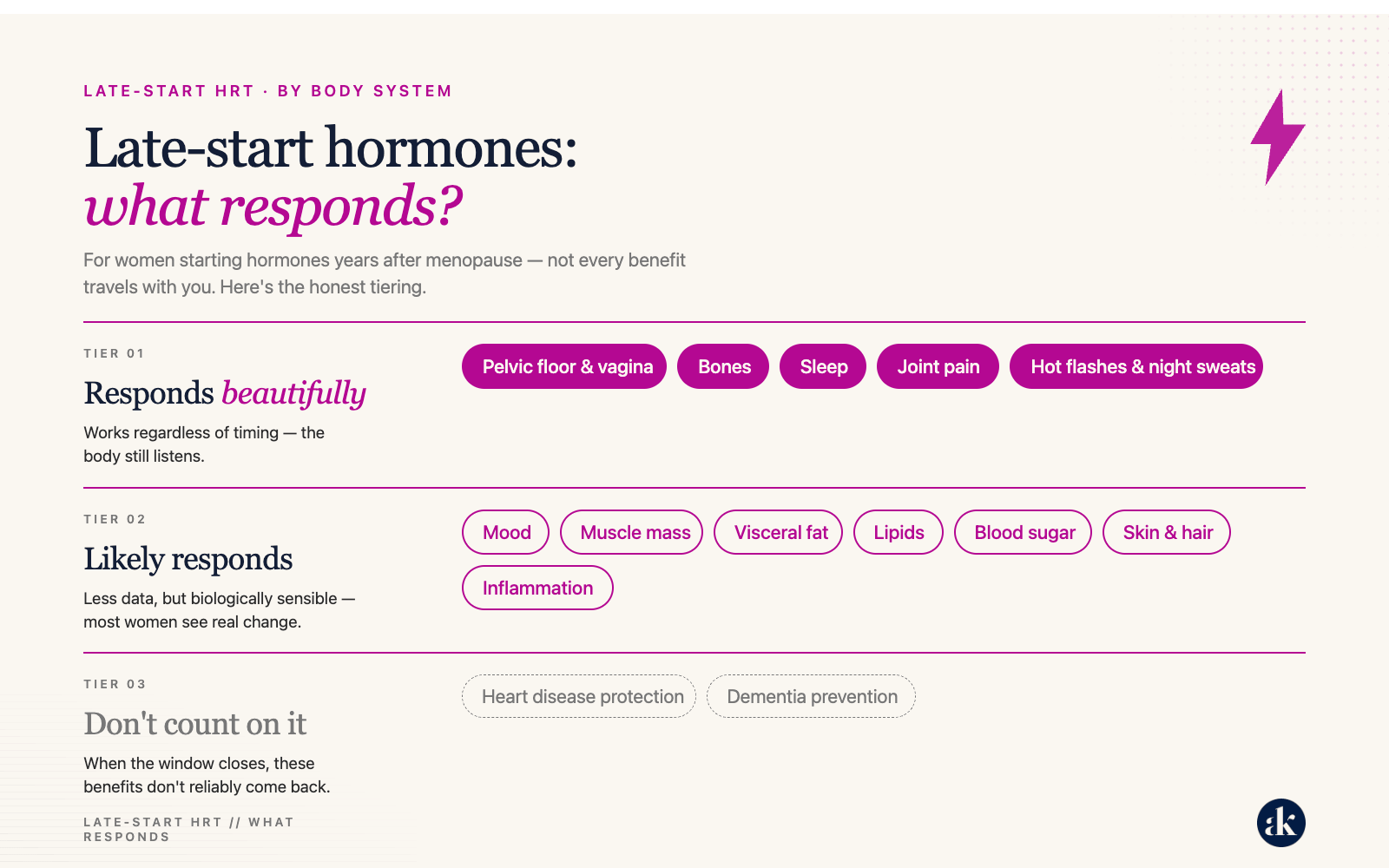
Here I have to level with you, because I refuse to sell you a fairy tale. Some parts of you respond beautifully no matter how long you waited. Others probably respond, though I have less hard data to wave around. And a couple of things simply will not show up to the party if you start late, no matter how nicely you ask. The second chart sorts the whole thing out, but here’s the gist.
Responds Beautifully: Your pelvic floor, your bones, your joints, your sleep, and your hot flashes are the reliable wins. These tissues respond to estrogen because they’re studded with estrogen receptors sitting there patiently, waiting, regardless of how many birthdays have stacked up. Bone is the headliner. Estrogen is still the single most effective tool we have for preventing fractures, and that held up in studies where the average woman was already in her sixties, well past the so-called window. Given that a broken hip at 80 is genuinely life-threatening, that is not a footnote.
May respond: The middle group (your skin, your mood, your muscle, your belly fat, your cholesterol, your blood sugar) very likely benefits too. The biology all points the right direction. I just can’t promise these the way I can promise the bone and pelvic floor wins, because we have fewer studies on women starting decades out. Think of it as a strong hunch backed by good chemistry rather than a signed contract.
Don’t count on it: And then the guests who won’t come when called: heart disease protection and dementia prevention. Started early, estrogen does both beautifully. Started fifteen years late, that ship has mostly sailed, and swallowed estrogen can even push stroke risk the wrong way. So we don’t start hormones late as a heart drug or a brain drug. Anyone promising you otherwise is selling something. The point isn’t that hormones quit working when you get older. It’s that they work for some things and not others, and knowing which is which keeps you smart instead of disappointed.
Summary:
So, one more time, for the woman in the back still quietly wondering if she missed her shot. You didn’t. Not entirely. You may have missed the chance to bank some bone and shield your arteries, and I’m sorry about that, because that window slamming shut was never your fault. But you have not missed the chance to sleep through the night, to stop dreading sex, to quit collecting bladder infections like loyalty points, or to feel like yourself in your own skin again.
Stop asking whether it’s too late. Ask what you’re after, then go get the right hormone for the job
Want more info on this subject?
I created a handy-dandy printable PDF all about Late-Start HRT? Get your Free Guide (see below), then share it with the women in your life. Let’s start changing how we think about late-start hormones in 60+ year old (still oh-so-fabulous) women!

HOT Tip: For a deeper dive into the published studies on late-start menopause hormone therapy, check out my previous article (see below). It includes links to all the key studies and provides more scientific detail. If you’re printing materials for your doctor, make sure to include both articles.

References:
Danan, E. R., C. Sowerby, K. E. Ullman, et al. “Hormonal Treatments and Vaginal Moisturizers for Genitourinary Syndrome of Menopause: A Systematic Review.” Annals of Internal Medicine (2024).
Gallo, K., C. A. Zhang, C. Burton, N. Kamdar, and E. A. Enemchukwu. “Vaginal Estrogen Utilization Among Medicare Beneficiaries With Genitourinary Syndrome of Menopause.” JAMA Network Open (2025).
Hamoda, H., S. Moger, E. Morris, et al. “Menopause Practice Standards.” Clinical Endocrinology (2024).
Pinkerton, J. V. “Hormone Therapy for Postmenopausal Women.” The New England Journal of Medicine (2020).
Committee on Clinical Practice Guidelines-Gynecology. “Management of Postmenopausal Osteoporosis: ACOG Clinical Practice Guideline No. 2.” Obstetrics and Gynecology (2022).
US Preventive Services Task Force, D. C. Grossman, S. J. Curry, et al. “Hormone Therapy for the Primary Prevention of Chronic Conditions in Postmenopausal Women: US Preventive Services Task Force Recommendation Statement.” The Journal of the American Medical Association (2017).
Eastell, R., C. J. Rosen, D. M. Black, et al. “Pharmacological Management of Osteoporosis in Postmenopausal Women: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology and Metabolism (2019).
Lambrinoudaki, I., E. Armeni, N. Milli, and P. Anagnostis. “Then and Now: What We Have Learned From the WHI.” The Journal of Clinical Endocrinology and Metabolism (2026).
Gulati, M., E. Dursun, K. Vincent, and F. E. Watt. “The Influence of Sex Hormones on Musculoskeletal Pain and Osteoarthritis.” The Lancet Rheumatology (2023).
Williams, J. A. E., M. Chester-Jones, C. Minns Lowe, et al. “Hormone Replacement Therapy (Conjugated Oestrogens Plus Bazedoxifene) for Post-Menopausal Women With Symptomatic Hand Osteoarthritis: Primary Report From the HOPE-e Randomised, Placebo-Controlled, Feasibility Study.” The Lancet Rheumatology (2022).
Piérard, G. E., P. Humbert, E. Berardesca, et al. “Revisiting the Cutaneous Impact of Oral Hormone Replacement Therapy.” BioMed Research International (2013).
Hall, G., and T. J. Phillips. “Estrogen and Skin: The Effects of Estrogen, Menopause, and Hormone Replacement Therapy on the Skin.” Journal of the American Academy of Dermatology (2005).
Majidian, M., H. Kolli, and R. L. Moy. “Management of Skin Thinning and Aging: Review of Therapies for Neocollagenesis; Hormones and Energy Devices.” International Journal of Dermatology (2021).
El Khoudary, S. R., B. Aggarwal, T. M. Beckie, et al. “Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association.” Circulation (2020).
Salpeter, S. R., J. M. Walsh, T. M. Ormiston, et al. “Meta-Analysis: Effect of Hormone-Replacement Therapy on Components of the Metabolic Syndrome in Postmenopausal Women.” Diabetes, Obesity & Metabolism (2006).
US Preventive Services Task Force, C. M. Mangione, M. J. Barry, et al. “Hormone Therapy for the Primary Prevention of Chronic Conditions in Postmenopausal Persons: US Preventive Services Task Force Recommendation Statement.” The Journal of the American Medical Association (2022).
Newman, C. B., M. J. Blaha, J. B. Boord, et al. “Lipid Management in Patients With Endocrine Disorders: An Endocrine Society Clinical Practice Guideline.” The Journal of Clinical Endocrinology and Metabolism (2020).
Sriprasert, I., S. S. Kim, I. E. Mohammed, et al. “Effect of Hormone Therapy on Lipoprotein Subfractions in Early and Late Postmenopausal Women.” The Journal of Clinical Endocrinology and Metabolism (2025).
Samaras, K., C. S. Hayward, D. Sullivan, R. P. Kelly, and L. V. Campbell. “Effects of Postmenopausal Hormone Replacement Therapy on Central Abdominal Fat, Glycemic Control, Lipid Metabolism, and Vascular Factors in Type 2 Diabetes: A Prospective Study.” Diabetes Care (1999).
Menzies, C., R. Bowtell, N. Shur, and M. S. Brook. “Menopause, Female Sex Hormones, Skeletal Muscle Mass and Muscle Protein Turnover in Humans.” Journal of Cachexia, Sarcopenia and Muscle (2026).
Österdahl, M. F., M. Ni Lochlainn, C. Welch, et al. “Systematic Review on the Relationship Between Menopausal Hormone Replacement Therapy, Sarcopenia, and Sarcopenia-Related Parameters.” Maturitas (2025).
Javed, A. A., A. J. Mayhew, A. K. Shea, and P. Raina. “Association Between Hormone Therapy and Muscle Mass in Postmenopausal Women: A Systematic Review and Meta-Analysis.” JAMA Network Open (2019).
Kim, S. W., and R. Kim. “The Association Between Hormone Therapy and Sarcopenia in Postmenopausal Women: The Korea National Health and Nutrition Examination Survey, 2008-2011.” Menopause (2020).
Glynne, S., A. Kamal, L. McColl, et al. “Transdermal Oestradiol and Testosterone Therapy for Menopausal Depression and Mood Symptoms: Retrospective Cohort Study.” The British Journal of Psychiatry (2026).
Brown, L., M. S. Hunter, R. Chen, et al. “Promoting Good Mental Health Over the Menopause Transition.” The Lancet (2024).
Gordon, J. L., D. R. Rubinow, T. A. Eisenlohr-Moul, et al. “Efficacy of Transdermal Estradiol and Micronized Progesterone in the Prevention of Depressive Symptoms in the Menopause Transition: A Randomized Clinical Trial.” JAMA Psychiatry (2018).
Bofill Rodriguez, M., L. N. Yong, S. Mirkov, et al. “Long-Term Hormone Therapy for Perimenopausal and Postmenopausal Women.” The Cochrane Database of Systematic Reviews (2025).
Chlebowski, R. T., A. K. Aragaki, K. Pan, et al. “Estrogen Plus Progestin and Colorectal Cancer: Long-Term Findings From the Women’s Health Initiative Randomized Clinical Trial.” Journal of Clinical Oncology (2024).
Nakhostin, L., A. Stadler, and P. Stute. “Impact of Menopausal Hormone Therapy on Colorectal Cancer Risk: A Systematic Review.” Clinical Endocrinology (2021).
Gartlehner, G., S. V. Patel, S. Reddy, et al. “Hormone Therapy for the Primary Prevention of Chronic Conditions in Postmenopausal Persons: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force.” The Journal of the American Medical Association (2022).
Chandrasekhar, J., J. Yao, S. Gong, et al. “Cardiovascular Health in Women: Across the Lifespan.” Clinical Endocrinology (2026).
Langhe, R., T. Kelly, R. Ibrahim, et al. “The Role of Hormone Replacement Therapy in the Management of Perimenopausal Mental Health Symptoms: A Narrative Review.” International Journal of Gynaecology and Obstetrics (2026).
Bodner-Adler, B., M. Alarab, A. M. Ruiz-Zapata, and P. Latthe. “Effectiveness of Hormones in Postmenopausal Pelvic Floor Dysfunction: International Urogynecological Association Research and Development Committee Opinion.” International Urogynecology Journal (2020).
“Estrogen and Progestogen Therapy in Postmenopausal Women.” Fertility and Sterility (2006).
I got started on E, P, T at the end of “the window.” By end, I mean photo finish - ten years post-meno and 59 yo. I’ve reaped all the benefits - like the full menu. My parents lived until 95 (dad) and 102 (mom). So I’d like to think that at 59, I am just hitting middle age. ;)
Thank you for always sharing useful information! Also, the calendar numbers and days of the week killed me.